
A thought leadership article for the plastic and reconstructive surgery community | Advanced Biomedical Concept | June 2026
Ask any experienced breast surgeon about autologous fat grafting and you’ll hear something like this: it works beautifully when it works. The outcomes, when they’re good, are genuinely good – natural, soft, biocompatible, the patient’s own tissue. But the when is the problem. Fat grafting has carried a persistent qualification attached to every one of its results: it depends.
It depends on the harvest site. It depends on the processing technique. It depends on the volume transferred, the recipient site vascularity, the patient’s BMI, the number of passes. And the evidence bears this out: reported volume retention rates in breast autologous fat grafting range from 30% to 80% across the literature.¹
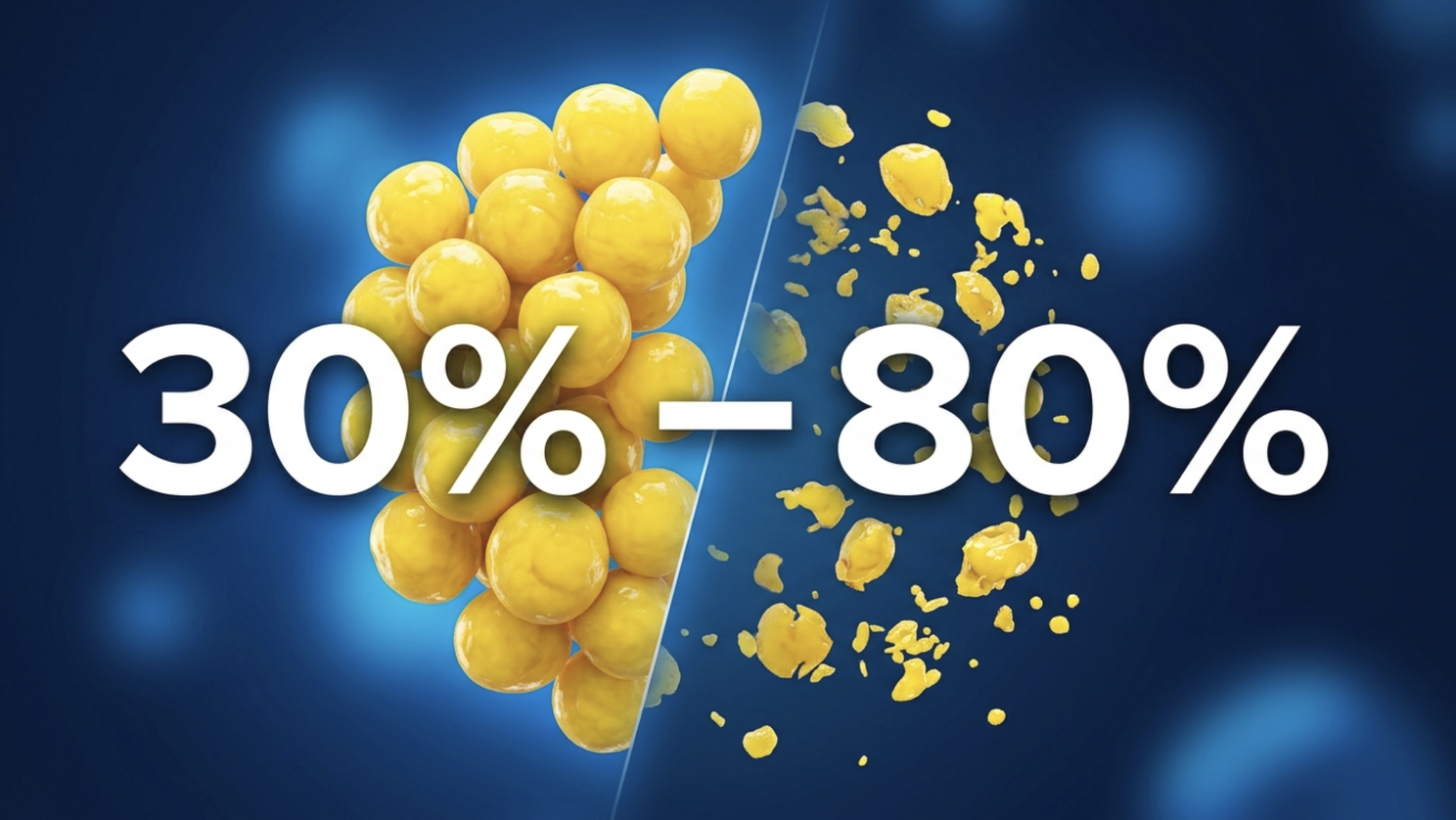
An average of around 58%.¹ In a reconstructive setting, that variability isn’t a clinical footnote – it’s the reason patients come back for a second session, a third, sometimes more. The average number of procedures for breast reconstruction patients undergoing fat grafting is 3.4.²
That number represents real costs. Real OR time. Real patient burden. And – if we’re honest – a real ceiling on how widely fat grafting can be adopted as a reliable, scalable reconstructive and aesthetic tool.
This is the retention problem. And it’s largely a process problem.
Why Fat Dies
The biology of fat grafting failure is well understood. Liposuction disrupts the vascular architecture of aspirated adipose tissue – blood flow to the graft site is severed at harvest.³ From that moment, the graft is in a race against ischaemia. Whether it survives in the new location depends on how quickly revascularisation occurs, and on how much biological damage was done to the adipocytes and their supporting stromal cells before transfer.

The processing step – what happens between harvest and injection – is where surgeons can either protect the graft or compromise it further. Centrifugation, still the most commonly used purification method, applies mechanical force that damages adipocyte membranes and reduces cell viability.⁴ Studies comparing processing techniques consistently show that cell structure destruction and viability decline are more evident in centrifugation groups than in filtration-based approaches.⁴ Alongside the cellular damage, centrifugation concentrates oil – the byproduct of lysed adipocytes – and does not reliably remove red blood cells or the inflammatory mediators that accelerate fat necrosis.
Fat necrosis is the most common complication in breast fat grafting, representing 43.7% of all complications in a comprehensive review of breast augmentation with autologous fat.² Its triggers are well-documented: ischaemia, poor graft dispersion, and inflammatory contamination in the transferred material. All three are influenced by processing quality.
The processing step, in other words, is not a neutral step in the fat grafting workflow. It is where the outcome is partly determined before the surgeon places the first injection.
The Standardisation Gap
Beyond the biology, there is a systems problem. Fat grafting, as practised today across most institutions, is not a standardised procedure. The harvest technique, the processing method, the cannula choice, the injection volume per pass – these vary between surgeons, between departments, and sometimes between cases performed by the same surgeon. Published evidence reflects this: when outcome data varies as widely as 30–80% for the same procedure, part of what’s being measured is process variation, not just biological variability.
A 2024 systematic review on maximising longevity and volume retention of fat grafts identified the processing technique as one of the most modifiable factors influencing outcome.⁵ The evidence increasingly points to filtration-based purification – which removes contaminants through a membrane rather than applying destructive centrifugal force — as superior for preserving adipose tissue viability and structural integrity.⁴

The implication for clinical practice is significant. If a meaningful portion of fat grafting variability is process-driven rather than biology-driven, then standardising the process should produce more consistent outcomes. The question is: which system, and how?
What Breast-Specific Engineering Requires
Not all fat grafting systems are designed with breast surgery in mind. The volumes involved in breast reconstruction and augmentation — often 200–400ml or more for large-volume grafting — place demands on a purification system that smaller-volume aesthetic applications don’t face. The port geometry, the membrane pore size, the processing time, the ability to scale from subtle contouring to full-volume reconstruction without changing methodology: these are breast-specific engineering requirements.
They matter because the breast is not an interchangeable recipient site. Its vascular density, tissue compliance, and anatomical constraints – particularly in post-mastectomy reconstruction, where fibrosis and radiation changes may be present – create conditions where graft quality at the point of injection matters enormously. A system optimised for facial fat grafting, or engineered without a specific anatomical context, is not the same as one designed from the ground up for breast tissue.
Fat lobule size is one example of where this specificity shows up in practice. Evidence supports harvesting fat in smaller lobule sizes to maximise the surface-area-to-volume ratio available for early diffusion-based nutrition before revascularisation — the critical window for graft survival. Optimising port geometry for consistent harvest of lobules under 3mm in diameter is a design choice that reflects this biology, not a marginal engineering detail.
Patient Satisfaction Is High — When It Works
It is worth pausing on what the positive evidence shows, because it sets the bar for what consistent fat grafting could achieve.
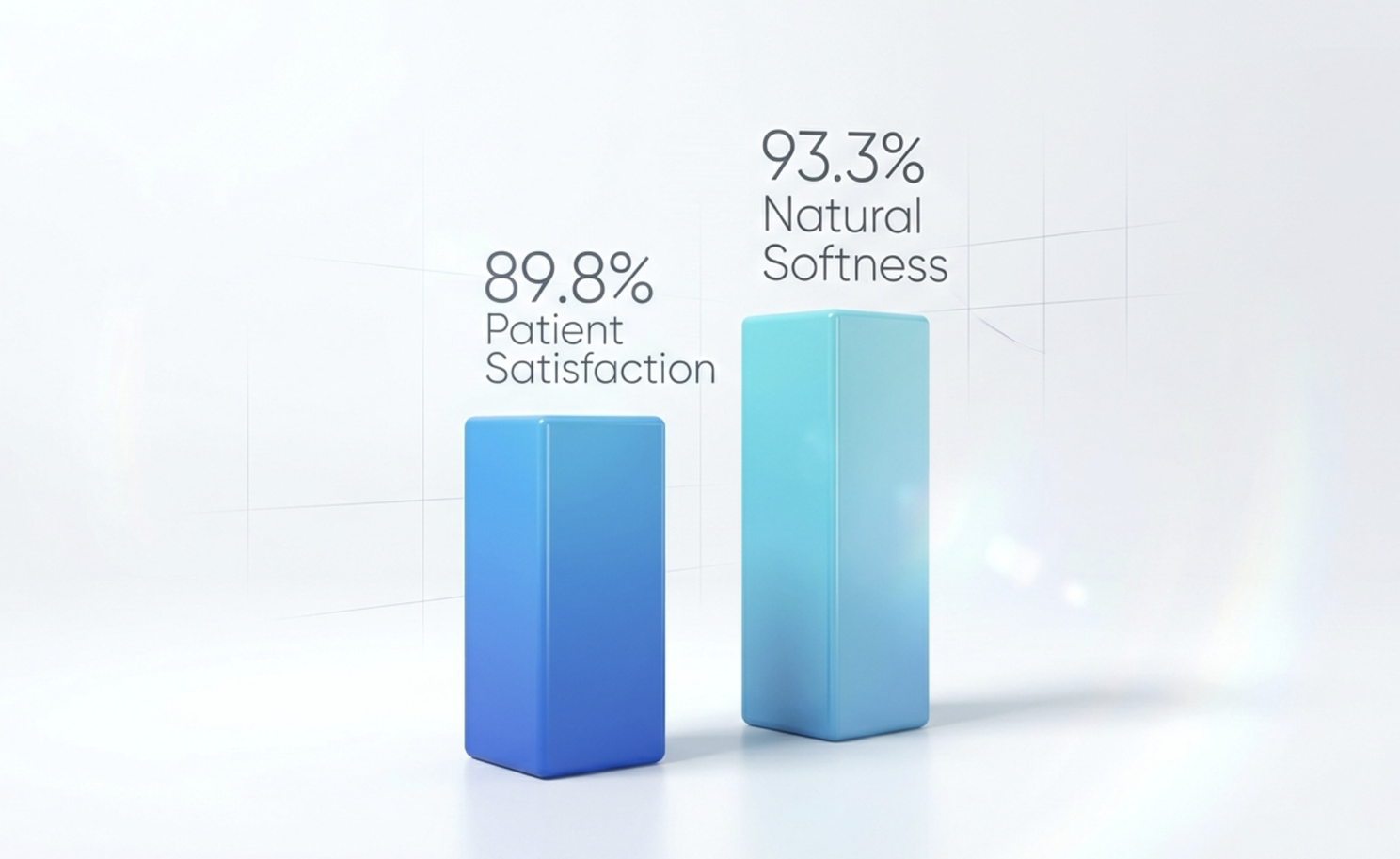
In a 2024 study on immediate oncoplastic breast reconstruction with fat grafting, 89.8% of patients were satisfied with their outcomes at six months — with no major complications or readmissions in the 30-day postoperative period.² Patient satisfaction scores in long-term follow-up of fat grafting breast procedures reach 88.3/100 for surgical results and 93.3/100 for breast softness.⁶ The biology of autologous tissue — when the graft survives — produces results that implant-based reconstruction consistently struggles to match on softness, naturalness, and patient-reported experience.
The argument for improving fat grafting is not that it is a poor procedure. It is that the gap between its best results and its average results is too large, and that the process is too variable for it to reach its full clinical and patient potential.
Where Fat Dialysis Fits In
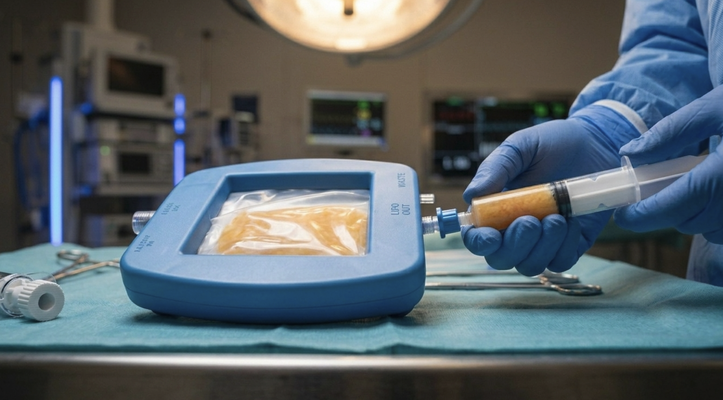
The concept behind Fat Dialysis — a continuous, active, gentle washing-filtration process using a semi-permeable microfiltration barrier — applies the same principle that filtration research supports: remove the contaminants (oil, blood, inflammatory triggers) without damaging the cells you want to keep.
What makes this relevant to the standardisation problem is not just the purification outcome but the process consistency. When the same tools, the same methodology, and the same technique are applied in every case, the graft going into the patient is as uniform as the biology allows it to be. The variable being removed is the processing variable — the difference between how one surgeon handles fat and how another does.
That is the contribution that process standardisation makes to fat grafting outcomes. Not a guarantee. Not a cure for the biology of ischaemia or the challenges of radiation-damaged recipient tissue. But a meaningful reduction in the preventable variability — the kind that comes from the processing step, not the patient’s anatomy.
The Standard Worth Setting
Fat grafting has earned its place in the reconstructive and aesthetic breast surgery toolkit. What it hasn’t yet achieved is the consistency that would make it the first-line option for a broader range of patients and institutions. That consistency starts with the process.
If we agree that the processing step materially influences outcomes – and the evidence is clear that it does — then the question becomes which process we standardise around, and why. That answer should be driven by the same standard we apply to everything else in medicine: what does the evidence support, reproducibly, at scale?
At Advanced Biomedical Concept, that’s the question we built EXAFAT around.
Discover how the fat grafting system works—read more about Exafat here.
References
- Volume retention rate after breast autogenous fat grafting and related influencing factors: A systematic review and meta-analysis. Journal of Plastic, Reconstructive & Aesthetic Surgery, 2023. https://www.sciencedirect.com/science/article/abs/pii/S1748681523007829
- Immediate Oncoplastic Breast Reconstruction with Fat Grafting: Preliminary Radiological, Aesthetic, and Patient Satisfaction Outcomes. PMC, 2025. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12423156/
- Advancing fat graft survival: from adipose-derived stem cell mechanisms to next-generation regenerative strategies. Frontiers in Cell and Developmental Biology, 2026. https://www.frontiersin.org/journals/cell-and-developmental-biology/articles/10.3389/fcell.2026.1870729/full
- Comparative Analysis of a New Automatic System and Four Existing Techniques for Autologous Fat Grafting. Plastic and Reconstructive Surgery – Global Open, 2023. https://pmc.ncbi.nlm.nih.gov/articles/PMC10578716/
- Maximizing the Longevity and Volume Retention of Fat Grafts: Advances in Clinical Practice. PMC, 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12368828/
- Exploring the Role of Autologous Fat Grafting in Implant-Based Breast Reconstruction: A Systematic Review of Complications and Aesthetic Results. PMC, 2025. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12193874/
© Advanced Bio Concept 2026. This article is intended for healthcare professionals. Clinical data referenced is from peer-reviewed published literature and does not constitute a guarantee of individual device or procedure outcomes. All promotional use of clinical data is subject to regulatory review.